Penile Implants
A penile implant (also called a penile prosthesis) is a surgically placed, mechanical device that helps a man get an erection—and keep it—for as long as he likes. It’s one of several treatment options for men with erectile dysfunction (ED). And it has high satisfaction rates.
Still, men need to weigh some important pros and cons before getting an implant. Read on to learn more about the different types of implants, the surgery involved, and what men can expect afterward.
Why do men choose penile implants?
Erectile dysfunction—the inability to get an erection firm enough for sex—is a common problem. While there are several treatments available, such as pills, self-injections, and vacuum devices, they’re not suitable for all men. For example, men who take nitrates for heart conditions cannot use ED medications because of a dangerous drug interaction.
Success with ED treatments can vary, too. What works for one man may not work for another. Generally, men try other ED treatment options before deciding on an implant.
Men with Peyronie’s disease may also get penile implants. This condition causes the penis to bend, sometimes to a point where intercourse becomes quite difficult. An implant can straighten the penis and help with any erection problems.
Transgender men may get penile implants as they undergo gender affirmation surgeries. During these procedures, surgeons create a penis and may implant a prosthesis to aid sexual activity.
Types of penile implants
In general, there are two different types of implants:
Inflatable implants
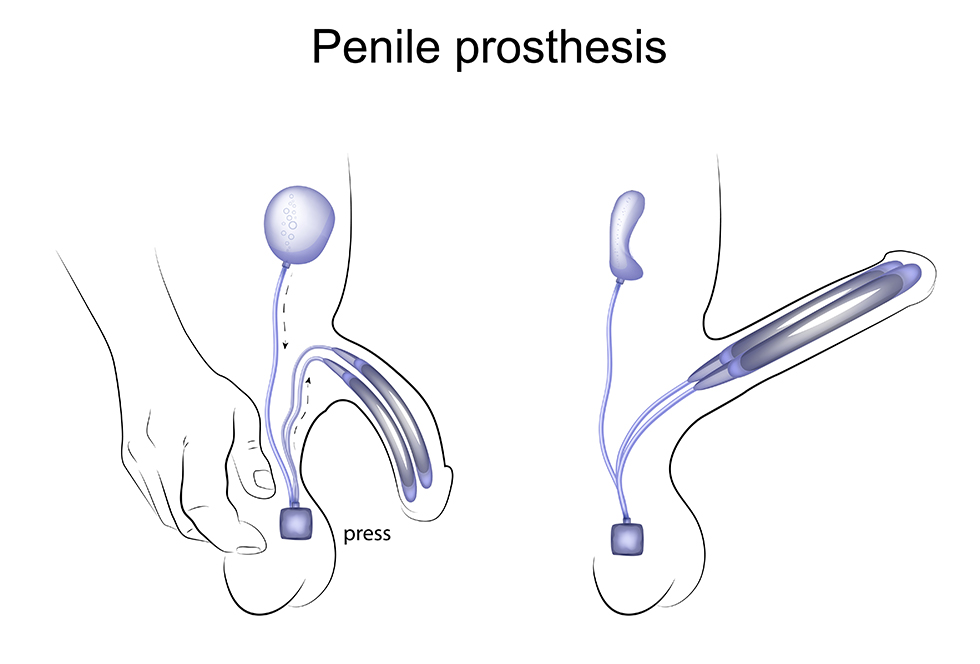
The most common type of implant is a 3-piece inflatable implant. The three parts are connected by tubes. They include:
- A pair of inflatable cylinders that are inserted into the shaft of the penis
- A fluid-filled reservoir placed in the abdomen
- A pump placed in the scrotum
When a man wishes to have an erection, he simply activates the pump in his scrotum. Saline fluid from the reservoir then moves into the cylinders and inflates them, creating the erection. When the man is done with sexual activity, he presses on the pump again. The cylinders deflate and the fluid moves back to the reservoir.
A 2-piece inflatable implant is also available, but it’s less common. This type works in a similar way, but the reservoir and the pump are in the same piece.
Malleable (semirigid) implants
These implants are flexible silicone rods that are inserted into the penis. When a man wants an erection, he can simply lift his penis up into position, then move it back down when he is finished with sexual activity. Malleable implants are not common nowadays, but they might be suitable for men who may have trouble activating a pump in the scrotum.
Advantages of penile implants

- The man has full control. A man can get an erection and keep its firmness for as long as he likes. He can also have as many erections in a day as he wishes.
- They have high satisfaction rates. Studies have shown that the satisfaction rate among men with 3-piece implants is 90% or higher.
- Sex can be more spontaneous. A man does not have to worry about timing the dose of a pill or stopping sexual activity to give himself an injection or use a vacuum device. Instead, he can create an erection in the moment.
- Implants last for years. Some men get 15 to 20 years of use from the same implant before it needs replacing.
- They’re discreet. The penis looks natural. People usually can’t tell if a man has an implant by looking at his penis. (Malleable implants may be an exception, as the penis is always somewhat firm.) During intercourse, partners usually cannot tell that a man has an implant.
- They don’t affect sexual desire or performance. For most men, sexual sensations, ejaculation, and orgasms feel the same as they did before the implant.
- They may boost a man’s sexual confidence. Men may feel less anxious about intimacy knowing that they can get a firm erection every time they have intercourse.
A man can get an erection and keep its firmness for as long as he likes.
Disadvantages of penile implants
- A surgical procedure is involved. Like any surgery, penile implant surgery has risks, such as infection, bleeding, and injury to surrounding areas. However, surgeons take special precautions to lower the risk of complications. Infection rates are estimated to be 1% to 2%. If there is an infection, the device is usually replaced.
- Implants can malfunction. There are times when a penile implant can malfunction, although this is rare.
- They are permanent. Because of the nature of implant surgery, a man can no longer have natural erections once he has an implant. Other ED treatments, such as pills or injections, will no longer be options.
What happens during penile implant surgery?
Before surgery, a man’s doctor will tell him how to prepare. The man may receive special instructions for taking medications or supplements, eating and drinking, and bathing beforehand.
The surgery itself is performed under general anesthesia and takes about one to two hours. It may be done as an outpatient procedure, and many men can go home the same day. However, some men may need to spend a night in the hospital.
To implant the device, the surgeon makes a small incision in the genital area. The inflatable cylinders (or bendable rods, if a malleable implant) are inserted into the shaft of the penis. If it is a 3-piece inflatable device, small incisions are made so that the reservoir can be placed in the abdomen and the pump can be placed in the scrotum. The pieces are then connected and the incisions are closed. The man may have a temporary surgical drain.
Men having implant surgery will need to have someone drive them home. They should also have someone stay with them for the first day or two.
Note: Not all men are good candidates for implant surgery. Men who are at higher risk for complications and those who have heart disease or poorly managed diabetes may not be able to have surgery.
Recovering from penile implant surgery
Back at home, men recovering from implant surgery may experience swelling, pain, or discomfort for the first week. These symptoms may be managed with medicines and ice packs. If there is a drain, it will be removed in the first few days after the procedure.
Men will need to avoid heavy lifting and vigorous activity, including exercise, for up to four weeks. If they work a desk job, they can return to work after a week or so. Men with more physical jobs may need to wait up to four weeks before returning to work.
Sex—both intercourse and masturbation—will need to wait four to six weeks while the body heals. At this time, the man’s doctor will teach him how to use the implant.
Men who have the following symptoms during recovery should call their doctor right away:
- Heavy bleeding
- Fever
- Worsening pain
- Infection
Adjusting to a penile implant
It may take time to adjust to sex with a penile implant. However, many men find that their sex life improves, knowing that they can now count on having a firm erection. Men who have problems with their device or have further questions should talk to their doctor.
Resources
Cleveland Clinic
“Penile Implants”
(Last reviewed: November 11, 2022)
https://my.clevelandclinic.org/health/treatments/10054-surgical-penile-implants
EAU Patient Information (European Association of Urology)
“Penile Implants”
https://patients.uroweb.org/treatments/penile-implants/
“Penile Implants”
https://patients.uroweb.org/penile-implants2/
Medscape
Hellstrom, Wayne John G., MD, FACS
“Penile Prosthesis Implantation”
(Updated: June 14, 2022)
https://emedicine.medscape.com/article/446761-overview
Urology Care Foundation (American Urological Association)
“Penile Implant”
https://www.urologyhealth.org/healthy-living/urologyhealth-extra/magazine-archives/spring-2020/insights-penile-implant-x8259
“What to Know about Penile Implants with Dr. Melissa Mendez”
(Urology Care Podcast. 2021)
https://www.urologyhealth.org/healthy-living/urology-care-podcast/sexual-health-podcasts/what-to-know-about-penile-implants-with-dr-melissa-mendez

